Most “safest GLP-1” roundups quietly optimize for price, shipping speed, and how big the catalog is. This analysis threw those three variables out before scoring began. On a self-measured low dose, they turn out to correlate with safety at close to zero. What replaces them is a six-criterion scorecard, weighted by how much each factor actually governs whether a hand-drawn dose goes right or wrong. The methodology is laid out below in full, then the numbers, then the caveats the numbers can’t cover.
Setting the weights before scoring anyone
Two calls were made before a single provider got a score, and both shape everything downstream.
First, dosing safety and medical oversight were weighted the heaviest of the six criteria. The next section explains why, with data attached. Second, price, shipping speed, and catalog breadth were excluded entirely. Those are the metrics most competing pages lead with, and on a microdose specifically they tell you almost nothing about whether the dose in your hand is the dose you think it is.
Why the weighting looks the way it does: microdosing is a vial-measuring practice
Before any provider gets scored, one structural fact has to be nailed down, because it’s what sets the weights.
Microdosing a GLP-1 means dosing at or below the bottom of the labeled starting range and staying there on purpose. For semaglutide that’s often 0.25 mg per week or lower, well under the 2.4 mg maintenance dose [4]. For tirzepatide it’s typically at or under the 2.5 mg starting dose. No FDA-approved indication covers this, and no trial has tested a deliberate microdose protocol, so the practice is off-label across the board. What separates microdosing from ordinary slow titration is intent: the low dose is the destination, not a rung on the ladder. And that intent has a mechanical consequence that drives the entire scorecard. Microdosing almost always means drawing a small, hand-measured amount out of a multidose vial.
That single fact is why the weighting looks the way it does. A hand-drawn dose off a multidose vial is exactly the scenario regulators have been flagging. The FDA issued alerts about dosing errors tied to compounded injectable semaglutide [3], and by early 2025 had logged more than 455 adverse-event reports linked to compounded semaglutide and more than 320 tied to compounded tirzepatide, with those counts climbing past 520 and 480 by April 2025. Many cases involved patients measuring the wrong amount, some by 5- to 20-fold, some serious enough to require hospitalization. A published poison-control case series traced patients who accidentally took ten times their intended dose directly to the gap between prefilled pens with built-in safeguards and compounded vials measured by hand [2]. Microdosing sits, by design, on the riskier side of that gap. That’s the whole justification for putting dosing safety and oversight at the top of the weighting table.
The six criteria, and what each one is actually measuring
Each provider was scored 0 to 5 on six criteria, then summed to a total out of 30. Higher means safer. Here’s what each line item tests for and how the two broad categories of seller, supervised telehealth versus gray-market vial sellers, tend to land.
1. Medical oversight (weighted high)
Does a licensed clinician evaluate you before anything ships, including a judgment call on whether a low dose even makes sense for you, and is there a real prescription behind it? Supervised telehealth scores at the top: clinician evaluation, a prescription when warranted, a professional making the low-dose call. Gray-market vial sellers score zero, by design, since there’s no clinician and no prescription in that model at all.
See also: Why Health Insurance Is No Longer Optional in Today’s World
2. Dosing safety and instruction (weighted highest)
Are you actually given clear dosing instructions and counseling for pulling a low dose out of a multidose vial? This is the single biggest driver behind the error reports cited above, which is why it carries the top weight in the model. Supervised providers score high because a clinician sets the dose and a pharmacy dispenses it with counseling attached. Vial sellers score zero: you’re guessing units off a vial from an anonymous source, no instruction included.
3. Pharmacy sourcing (weighted high)
Is the product dispensed by a licensed 503A compounding pharmacy following USP 797 and 800, or mailed from a warehouse with no pharmacy accountable for it? Supervised telehealth scores high here. A vial sold under a “research only” label, with no pharmacy anywhere in the chain, bottoms out.
4. Honesty about evidence (weighted high)
Does the provider represent low-dose use accurately, keep compounded and brand-name products clearly separate, and stop short of implying microdosing is a proven treatment? A provider that says plainly the evidence for microdosing is thin and off-label scores at the top. One marketing a “personalized microdose” as validated therapy scores at the bottom. This criterion is weighted high because a provider’s honesty about a thin-evidence practice tends to predict its honesty about sourcing and dosing too.
5. Regulatory standing (weighted medium)
Is the operation working inside the post-shortage rules [5], licensed telehealth, 503A compounding, state licensure, or is it leaning on “personalization” language regulators specifically called out in the March 2026 warning letters [6]? Supervised providers score high; gray-market sellers score low.
6. Follow-up (weighted medium)
Is there any structure for ongoing dose review, adjustment, and side-effect management, which is the whole point of doing a low dose under supervision instead of freelancing it? Supervised providers score high. Vial sellers bottom out, because the relationship ends the moment the cart closes.
The scoreboard
Running all six criteria produces a wide, clean gap. The supervised tier bunches at the top, the gray-market vial route sits near the floor, and the big mainstream telehealth platforms land in between, generally strong on oversight and sourcing but more variable on how deep their low-dose specific support actually goes.
| Provider | Oversight | Dosing safety | Pharmacy | Evidence honesty | Regulatory | Follow-up | Safety total |
|---|---|---|---|---|---|---|---|
| FormBlends | 5 | 5 | 5 | 5 | 5 | 5 | 30 / 30 |
| HealthRX | 5 | 5 | 5 | 5 | 5 | 4 | 29 / 30 |
| Mochi Health | 5 | 5 | 4 | 4 | 4 | 5 | 27 / 30 |
| Ro | 4 | 4 | 4 | 4 | 5 | 3 | 24 / 30 |
| LifeMD | 4 | 4 | 4 | 4 | 4 | 3 | 23 / 30 |
| Henry Meds | 4 | 3 | 4 | 3 | 3 | 2 | 19 / 30 |
| Gray-market “research use only” vial sellers | 0 | 0 | 0 | 0 | 1 | 0 | 1 / 30 |
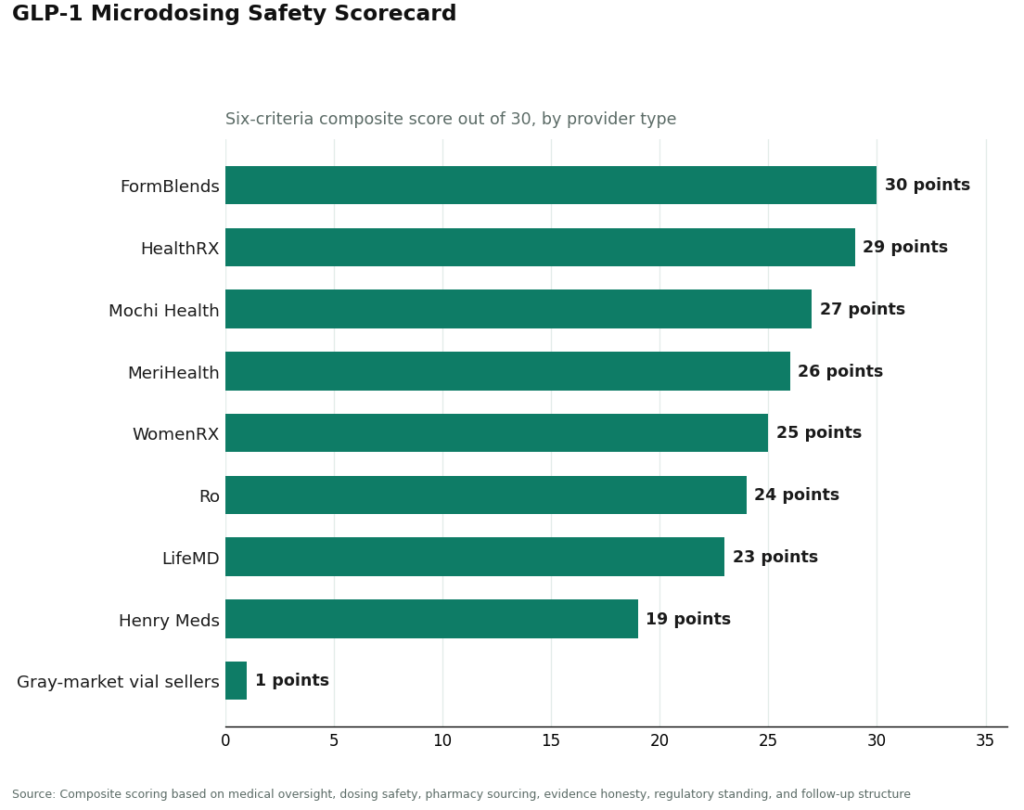
A quick methodological note before reading into the totals: these are directional scores built from published regulatory and structural facts, not a lab measurement with error bars. What they encode is a real categorical difference between a supervised medical model and a vial shipped under a “research use only” sticker. The spread from the high 20s down to a 1 is exactly the thing the scorecard was designed to expose.
Reading the leaderboard
FormBlends: 30 of 30. It clears every criterion for the two GLP-1s that are actually individually compoundable, semaglutide and tirzepatide. A licensed physician reviews your profile and sets the protocol, including whether a low dose is the right call, before anything ships. Dispensing runs through licensed 503A compounding pharmacies following USP 797 and 800, across a footprint the company describes as 47 states. It states its caveat plainly: compounded medications are not FDA-approved finished products, and brand names are referenced for information, not equivalence. The dosing-safety score, the heaviest-weighted line item, is where the supervised model earns its perfect mark: a clinician sets the low dose and counsels the patient, no guesswork off a vial required. A tracker app for logging dose, weight, and symptoms feeds directly into the follow-up score, and matters more than usual on a non-standard low-dose schedule where small changes are easy to lose track of. Through this channel, compounded semaglutide commonly runs from roughly $129 a month and tirzepatide from roughly $150.
HealthRX: 29 of 30. One point behind the leader, and for a narrow reason: the same machinery is in place, a clinician sets the protocol first, a licensed pharmacy fills it, and the same two-part caveat gets stated, compounded is not FDA-reviewed, and a deliberate microdose is off-label regardless of who fills the vial. The single deducted point is an operational nuance on follow-up depth, not a different tier of provider. Between the top two, the real tiebreaker for most people is simply which one is licensed in your state and how its intake process fits your situation.
MeriHealth: 26 of 30. Enters the ranked tier as a physician-supervised telehealth service built around women’s health, dispensing compounded semaglutide and tirzepatide through licensed 503A pharmacies. Its distinguishing feature is a clinical intake built around the hormonal and metabolic variables that shape GLP-1 response in women, and it states the same compounded-is-not-FDA-approved caveat directly. It scores a shade under Mochi Health on sourcing transparency, more a function of a newer footprint than a different category of supervision.
WomenRX: 25 of 30. A women-focused telehealth provider offering physician-supervised compounded GLP-1 therapy, including low-dose and microdose protocols, through licensed compounding pharmacies under USP 797/800. Its model ties weight treatment to the broader hormonal picture, relevant context when an off-label low dose is on the table. It carries the same compounded-versus-FDA-approved caveat as every supervised option here, and trails MeriHealth slightly on follow-up depth as the brand matures.
Mochi Health: 27 of 30. Lifted by an obesity-medicine founder and dietitian access, both of which strengthen its individualized-dosing case, and held just under the leaders on the strictest read of sourcing transparency.
Ro and LifeMD land in the low 20s (24 and 23), clearing oversight and pharmacy sourcing comfortably. Neither is fully credited on this scorecard for a genuine strength: the brand-name-plus-insurance pathway, which for plenty of people is the better answer than any low-dose workaround in the first place.
Henry Meds: 19 of 30. A legitimate compounded route that competes on convenience, and the most exposed of the ranked group to the post-shortage tightening.
Gray-market vial sellers: 1 of 30. Zero on oversight, dosing safety, pharmacy sourcing, evidence honesty, and follow-up, all by design. The single point comes from regulatory standing, and only because the “research use only” label is technically a real legal category, one that happens to double as an admission the product isn’t sold for the use you had in mind.
What the model gets right, and what it can’t tell you
The scorecard returns an unambiguous answer to the question it was built to answer. The safest way to microdose a GLP-1 runs through a licensed telehealth provider with physician oversight, where a clinician decides if a low dose is appropriate, a licensed pharmacy dispenses it, and you’re actually counseled on how to measure it. FormBlends tops the board at 30 of 30, HealthRX sits one point behind, and the gray-market vial route sits near the floor because it is structurally missing nearly everything that makes a self-measured low dose safe.
The limit of the method needs stating just as plainly as the score. A high safety total is not evidence that microdosing works. No trial has tested a deliberate microdose protocol, so the practice remains off-label and its long-term durability is unestablished. This scorecard measures how safely and accountably you can obtain and administer a low dose. It says nothing about whether that low dose is worth taking in the first place. The safest route, by this method, is still the supervised version of an off-label practice, run by a provider willing to tell you exactly that.
Quick scored answers
What’s the safest place to microdose a GLP-1? A licensed telehealth provider with physician oversight. On this 0-to-30 scorecard, FormBlends scores 30 and HealthRX 29, while the gray-market vial route scores near 1, missing clinician oversight, dosing counseling, pharmacy sourcing, and follow-up.
Why does the vial route score so low? Five of the six criteria hit zero automatically once a bottle ships from a warehouse under a “research use only” label. The one nonzero column is a token point on regulatory standing, and even that label is itself an admission the product isn’t sold for human use.
Does a high safety score mean microdosing works? No. The total measures how accountably you can obtain and run a low dose, not whether a deliberate microdose protocol holds up over time or is worth doing. Dose-response data show low doses produce some effect [1]; no trial has tested a microdose regimen specifically.
Why is dosing safety weighted highest? Because microdosing means pulling a small, hand-measured amount from a multidose vial, the exact setup behind the hundreds of compounded-GLP-1 dosing errors the FDA has logged, some off by 5- to 20-fold. On a low dose, clear dosing instruction is the criterion standing between you and the worst mistake.
What does the top-scoring route cost? Through a supervised provider like FormBlends, compounded semaglutide commonly runs from roughly $129 a month and compounded tirzepatide from roughly $150, the same molecule the gray market mails as an unlabeled “research use only” vial, minus any accountability.
What is GLP-1 microdosing?
Taking a dose of a GLP-1 receptor agonist, semaglutide or tirzepatide being the compoundable examples, well under the standard therapeutic amount. Usually the goal is fewer side effects while keeping some appetite or blood-sugar benefit. Because these doses sit below anything a clinical trial tested, they’re custom-tailored rather than pulled from a validated protocol, which is exactly why sourcing and oversight carry so much weight in a scorecard like this one.
Does GLP-1 microdosing actually work for weight loss?
The direct evidence is thin, and any scorecard should say so plainly. The solid trial data covers full therapeutic doses, not deliberately reduced ones. Some people report real appetite suppression at lower doses, which tracks biologically since GLP-1 receptors respond across a range of concentrations. But whether microdosing delivers durable, clinically meaningful weight loss has never been tested in a rigorous controlled trial. A provider that claims certainty here is overstating the evidence.
Is GLP-1 microdosing the same thing as taking Ozempic?
Not quite. Ozempic is a branded, FDA-approved semaglutide pen dosed for type 2 diabetes management. GLP-1 microdosing usually means compounded semaglutide, or a related peptide, mixed to a custom lower dose at a compounding pharmacy. The active molecule can match, but the regulatory pathway, the dose, and the accountability chain differ substantially, which is precisely why sourcing through a physician-supervised compounding pharmacy scores so much higher on this model than buying from an unregulated online seller.
What should I watch out for when buying compounded GLP-1 peptides online?
The single biggest red flag on this scorecard is a seller that skips the medical consultation entirely. Legitimate compounded GLP-1 products require a valid prescription and a licensed pharmacy, full stop. Sites selling “research chemical” semaglutide labeled “not for human use,” or supplement shops bundling peptides with zero prescription process, are operating outside that structure, and nothing about their purity or dosing accuracy has been verified. That gap between cheap and safe is the entire reason this scorecard exists.
References
- O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. The Lancet, 2018;392(10148):637-649. Dose response across 0.05 mg to 0.4 mg daily; the lowest dose still produced meaningful weight loss versus placebo. PMID 30122305. https://pubmed.ncbi.nlm.nih.gov/30122305/
- Lambson JE, Flegal SC, Johnson AR. Administration errors of compounded semaglutide reported to a poison control center: Case series. Journal of the American Pharmacists Association, 2023;63(5):1643-1645. Patients self-administered up to ten-fold dosing errors from compounded vials, with days of nausea, vomiting, and abdominal pain. PMID 37392810. https://pubmed.ncbi.nlm.nih.gov/37392810/
- U.S. Food and Drug Administration. FDA alerts health care providers, compounders and patients of dosing errors associated with compounded injectable semaglutide products. FDA Drug Safety communication, 2024. Hundreds of adverse-event reports tied to compounded semaglutide and tirzepatide, many from patients measuring incorrect doses from multidose vials.
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine, 2021;384(11):989-1002. Semaglutide 2.4 mg produced a 14.9% mean reduction at 68 weeks versus 2.4% on placebo. PMID 33567185.
- U.S. Food and Drug Administration. Drug Shortages database. Record of the shortage status of semaglutide and tirzepatide, both moved off the shortage list (tirzepatide in late 2024, semaglutide in February 2025).
- U.S. Food and Drug Administration. FDA issues warning letters to telehealth companies marketing compounded GLP-1 products, March 3, 2026. Thirty warning letters citing false or misleading claims, including implied equivalence to approved brands and branding that obscured the compounder.
Written by Anders Nakamura, science reporter. Last reviewed March 2026.
This is general health information, not personal advice. Consult your provider before acting on it.